
By Corey J. Langer, MD, ILCN Editor
Posted: April 16, 2020

Michele Carbone MD, Ph.D and colleagues have penned a far-ranging editorial, now published online in the Journal of Thoracic Oncology (JTO), on the “Facts, Myths, and Hypotheses” behind this pandemic and global public health crisis, which was first documented in Hubei Province in China. The advent of COVID-19 has clear cut implications for our patients with thoracic cancer, many of whom are immune-compromised or elderly, as well as for all of us in the health care profession. Carbone points out that the current incidence rates “barely scratch the surface” and that the real rates are likely far higher since testing material is not uniformly available. Nations that have made a major effort to test their citizens, unsurprisingly, are documenting much higher incidence than those, like the United States, that do not. In addition, early testing has been compromised by the faulty science in the design of some of the early PCR kits, leading potentially to “under-detection.” Recent ELISA kits have proven far more reliable and sensitive, and are now being used routinely in China and elsewhere. To date, no antiviral has shown any efficacy, and vaccines are thought to be 12 to 18 months off. So, at this point, scrupulous hygiene (proper hand-washing), screening at-risk individuals, and minimizing contact between those who have tested positive and the outside world until the disease has run its course are the optimal measures available.
In the early phase, patients exhibit fever, dry cough, and dyspnea. Like the 1918 Flu pandemic, SARS-CoV-2, can lead to rapid alveolar damage, which even ventilation and assisted oxygenation may not be able to overcome.
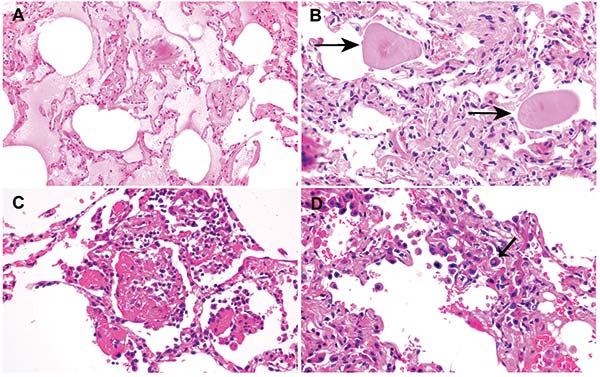
Finally, Carbone reviews the early pulmonary pathology observed in those with fulminant disease, which has all the earmarks of SARS (severe acute respiratory syndrome). In the early phase, patients exhibit fever, dry cough, and dyspnea. Like the 1918 Flu pandemic, SARS-CoV-2, can lead to rapid alveolar damage, which even ventilation and assisted oxygenation may not be able to overcome. Tian et al. in the JTO have documented the early pathology observed in two patients who had undergone lobectomies and who had GGOs in their lungs with COVID-19 documented on RT-PCR. Both patients ultimately became extremely ill, and one died. Edema and proteinaceous exudate were noted in the surgical specimens. In one case, abundant intra-alveolar pulmonary macrophages were present; alveolar walls or septa were expanded by proliferating fibroblasts with type II pneumocyte hyperplasia. Lung damage is not caused by the accumulation of granulocytes and fibrin, but by intra-alveolar organization and fibrosis. Radiographically, these patients will often first manifest peripheral GGOs near the pleura before more extensive consolidation occurs. ✦
IN REFERENCE TO:
Carbone M, Green JB, Bucci EM, and Lednicky JJ. Editorial: Coronaviruses: Facts, Myths and Hypotheses. J Thoracic Onc. 2020;doi: https://doi.org/10.1016/j.jtho.2020.02.024.
Tian S, Hu W, Niu L, Liu H, Xu H and Xiao S-Y. Pulmonary pathology of early phase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer. J Thoracic Onc. 2020; doi: https://doi.org/10.1016/j.jtho.2020.02.010.








{kind=link}